Since the spring of 2020, the COVID-19 pandemic has impacted nearly every sphere of life across the world. Healthcare systems, in particular, have been overwhelmed with massive surges of hospitalizations, and the burden of care for the nearly unprecedented volume of patients has fallen on the shoulders of healthcare workers (HCWs). To understand how American Muslim HCWs working in the United States have been impacted by this stress, and how they have been coping with it, this study surveyed nearly 700 American Muslim HCWs about one year into the pandemic. This report reveals that, while the detrimental impact of COVID-related stress and the compounded stress of discrimination was significant, American Muslim HCWs utilized several effective coping strategies, both religious and non-religious in nature.
Impact of COVID on Mental Health and Distress
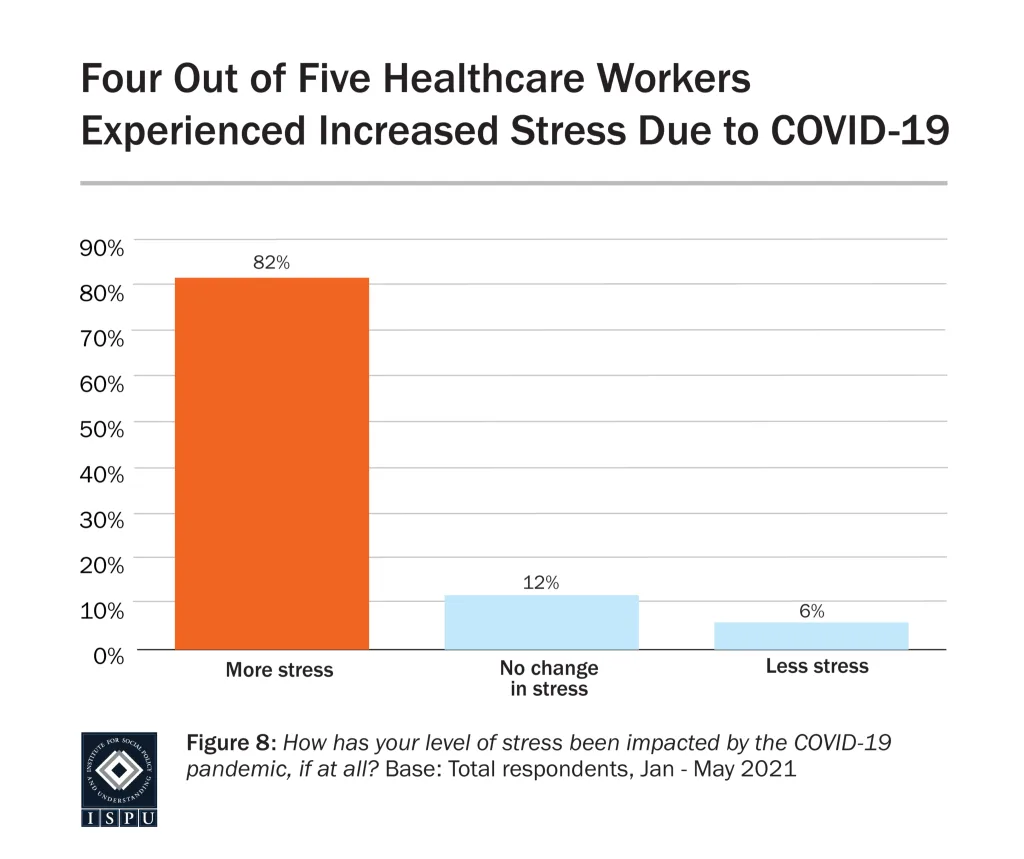
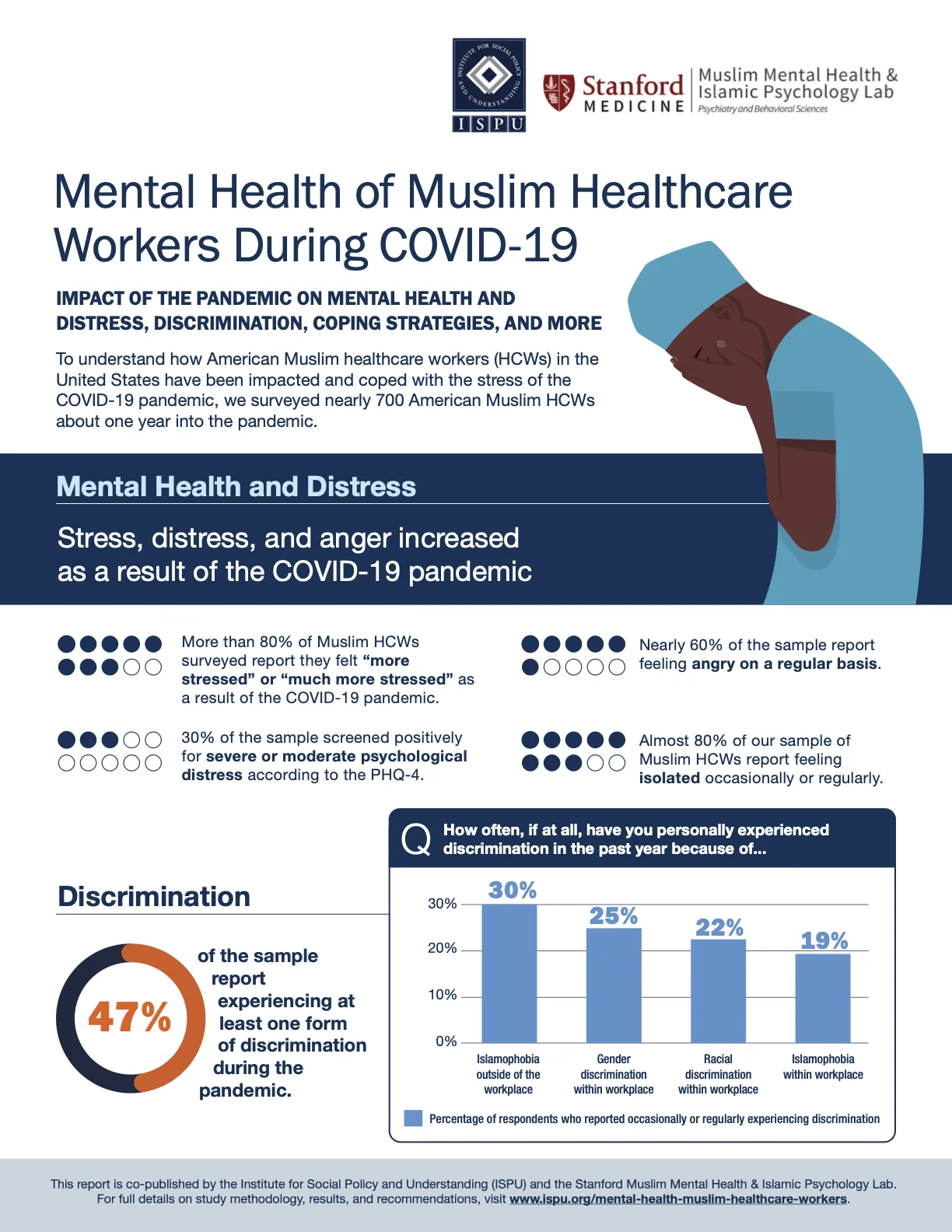
More than 80% of our study’s sample reported that they felt “more stressed” or “much more stressed” as a result of the COVID-19 pandemic. Additionally, about 30% screened positively for moderate or severe psychological distress according to the PHQ-4 (a short screening scale for anxiety and depression) and nearly 60% of the sample reported feeling angry on a regular basis. Concerningly, almost 80% of our sample reported feeling isolated occasionally or regularly. Given the vital role of factors such as family, community, and work environment to the population of interest to this study, this is particularly worrisome.
Frequency of Discrimination
Forty-seven percent of the overall sample reported experiencing at least one form of discrimination during the pandemic. Thirty percent of the sample reported experiencing Islamophobia occasionally or regularly outside of the workplace, and 19% reported experiencing Islamophobia within the workplace. In regard to racial discrimination within the workplace, 22% of those surveyed reported occasional or regular incidents. And, 25% reported experiencing gender discrimination within the workplace.
Discrimination Associated with Higher Risk of Psychological Distress, Including Depression and Anxiety
Our multivariate logistic regression analysis revealed that those HCWs who reported experiencing occasional or regular Islamophobia outside of the workplace in addition to racial discrimination within the workplace, compared to those who experienced no discrimination, had five times higher risk of mild psychological distress, and 6.6 times higher risk of moderate or severe psychological distress. HCWs experiencing occasional or regular discrimination of mixed forms (racial, gender, or religious), compared to those who experienced no discrimination, had five times higher risk of mild distress, and nine times higher risk of moderate or severe distress. This information is particularly concerning given that, in the absence of strong protective factors, these outcomes could be even further exacerbated. This sample, as discussed later in this report, utilized a number of widely protective coping strategies at a high rate, leading to the question of how HCWs who do not partake in those protective strategies may be even further impacted by experiences of discrimination.
Islamophobia in the Workplace Associated with Increased Healthy Coping Strategies, Particularly Those of a Religious Nature
We also found that those who reported experiencing Islamophobia within the workplace utilized a higher number of healthy coping strategies, particularly religious healthy coping strategies. Additionally, they were found to adopt fewer unhealthy coping strategies (more details on coping strategies will follow). It may be surprising that those who experienced Islamophobia were also more likely to use healthy coping strategies, given the detrimental effect of discrimination on the overall mental health of our participants. However, in light of existing research which shows that those who perceive Islamophobia tend to also view their religion as a more important part of their life, there may be a way to make sense of this finding.
Racial Discrimination in the Workplace Associated with Less Healthy Coping and More Unhealthy Coping
In contrast to the above finding, those healthcare workers who reported racial discrimination in the workplace were less likely to utilize healthy coping strategies and more likely to utilize unhealthy religious coping strategies. This finding raises several important questions, discussed further in the body of the report. Presently, our analysis cannot make conclusions about the cause of these paradoxical findings, but it illustrates that experiences of racial discrimination among our sample are linked with different patterns of coping compared to religious discrimination in the workplace. Continued research into the nuances of identity, discrimination, and stress response is definitely warranted to understand what may be at the root of this difference.
Most Common Coping Strategies
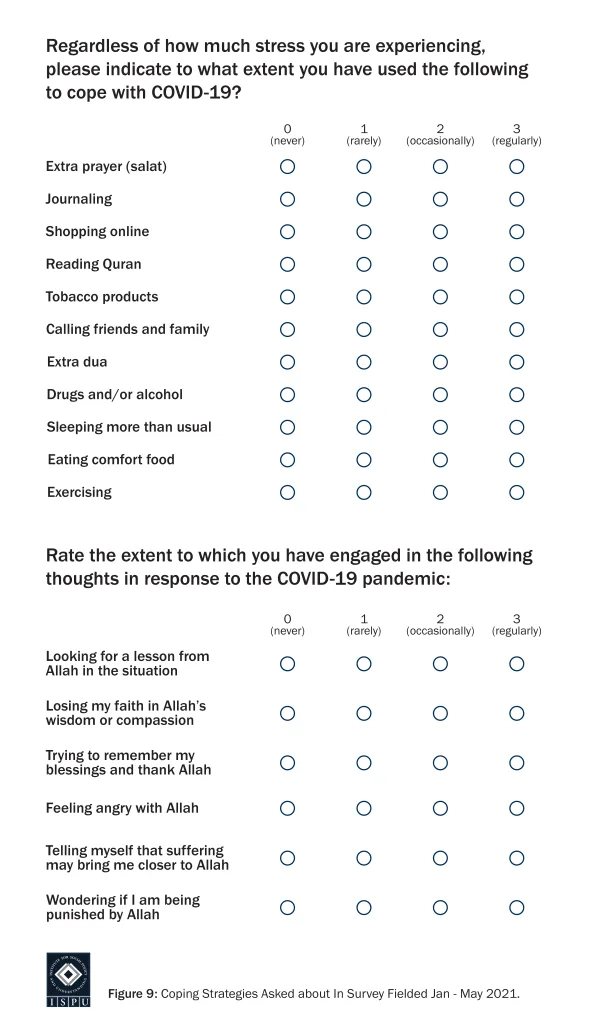
A coping strategy can be defined as a behavior a person partakes in or a belief a person relies on when dealing with stress, whether consciously or unconsciously, as an attempt to relieve their negative emotions. Our survey investigated numerous behavioral and cognitive coping strategies (see “Coping Strategies” for a comprehensive list). The most commonly used coping strategy reported in our sample was calling friends and family, with 82% of the sample reporting doing so occasionally or regularly. This demonstrates that this sample of American Muslim HCWs often leaned on their social support networks to help cope with pandemic-related stress. In our sample, the other most commonly utilized non-religious coping strategies were eating comfort food (79%), shopping online (62%), exercising (57%), and sleeping more than usual (51%). Religious coping strategies were used much more commonly than non-religious strategies as a whole, but extra du’aa (prayer of supplication or invocation) was particularly common (78%).
Some Coping Strategies Linked with Increased Risk of Distress
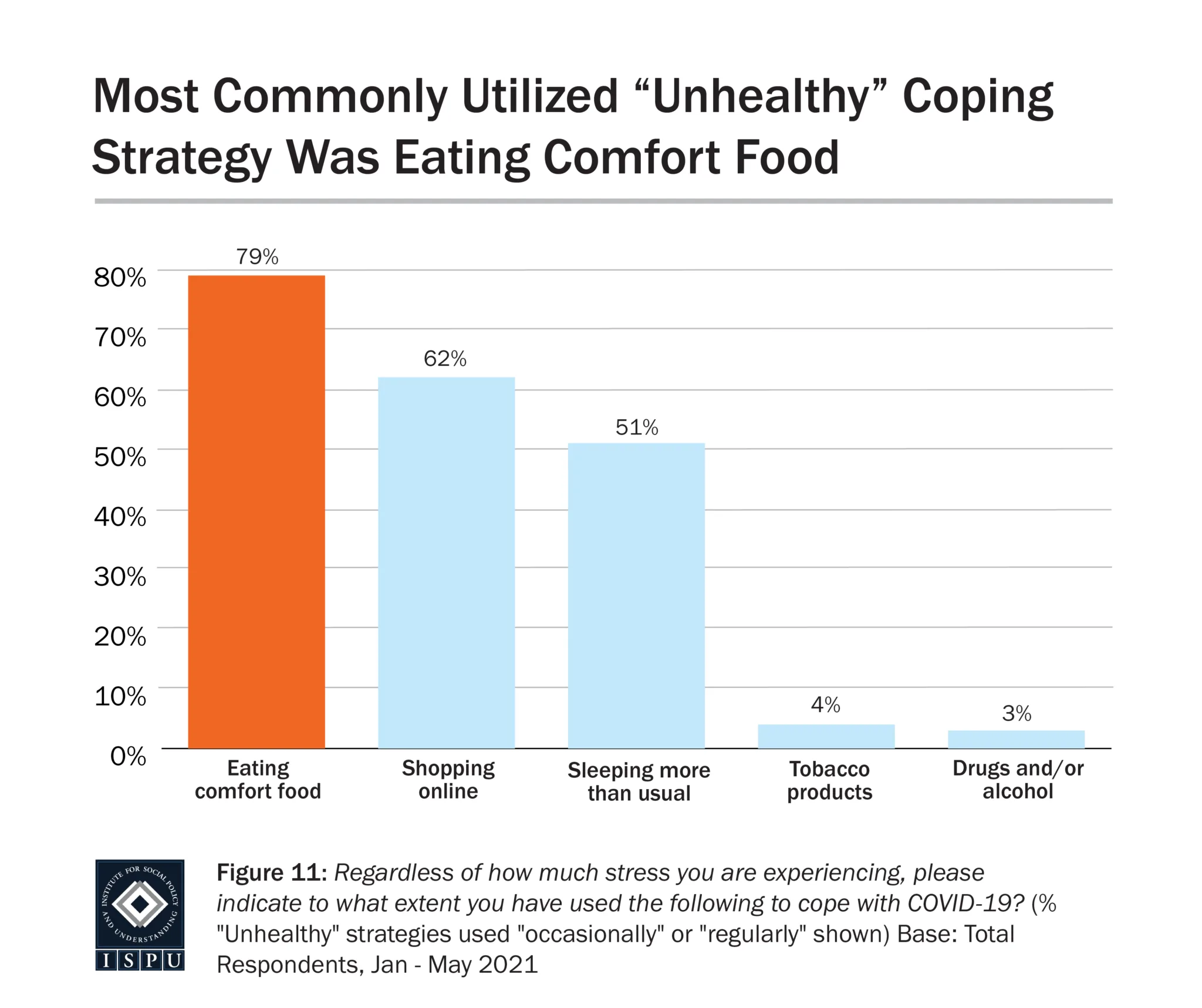
There are some coping strategies thought to be maladaptive, which have been linked to high psychological distress and lower overall mental health; this is in contrast with positive, or adaptive, coping strategies that can successfully relieve negative emotion and promote well-being (Mong & Noguchi, 2021). Some of these maladaptive, or unhealthy, coping strategies were observed in our sample, such as eating comfort food (79%), shopping online (62%), or sleeping more than usual (51%). Using multiple logistic regression analyses, all of these strategies had significant associations with poorer mental health, each being linked to more than two times increased risk of moderate to severe psychological distress as measured by the PHQ-4.
Feeling Angry with Allah was Strongly Linked to Feeling a General Sense of Anger on a Regular Basis and Risk for Depression
Muslim healthcare workers who reported thoughts of feeling angry with Allah were more than eight times more likely to also report feeling a general sense of anger on a regular basis. This reveals an opportunity for future research to investigate a potential link between anger inspired by environmental factors such as the pandemic and anger directed toward metaphysical/spiritual beliefs; however, our study alone cannot infer a link between these factors. Nevertheless, given the importance of religious beliefs and practices reported by our study’s sample, and the role of religious coping strategies highlighted in both our analyses and those of previous literature, the implications are significant for how American Muslim HCWs will be able to lean on their most effective methods of coping with stress.
Remembering Blessings and Thanking Allah was Widely Protective
In our study, those who reported trying to remember their blessings and thank Allah were at a significantly reduced risk for psychological distress, after controlling for other coping strategies, race, gender, and age. This was the most protective religious coping strategy revealed within our sample. American Muslim HCWs from our study reported utilizing gratefulness at a high rate (93%), indicating that this was a commonly held value. The protective impact of this strategy, on top of expansive existing literature about the positive impact of gratefulness, points to another major strength among American Muslim HCWs. Alongside our finding about calling friends and family (used by over 80% of participants), our study reveals a strong tendency for American Muslim HCWs to utilize healthy coping strategies that are well-supported by existing evidence. These strategies can be capitalized on and encouraged among American Muslim HCWs to further protect against the stresses of their role, particularly amidst a pandemic.
Seeing a Mental Health Professional During the Pandemic was Widely Protective
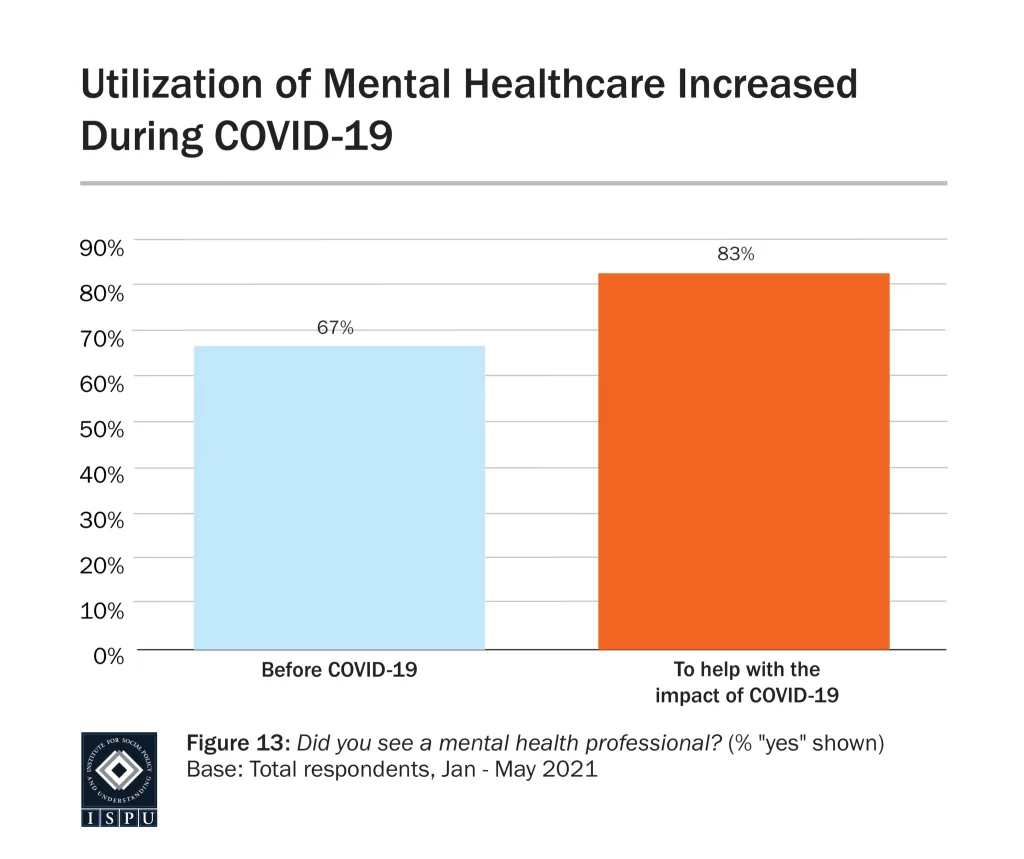
Eighty-three percent of our sample reported seeing a mental health professional “to help with the impact of COVID-19.” This is a very high proportion, particularly given previous evidence that western Muslims overall have underutilized mental healthcare (Zia et al., 2013). Additionally, our regression analysis found that seeing a mental health professional during the pandemic was determined to be protective against feeling angry, screening positively for depression, anxiety, and mild and moderate psychological distress. It is hoped that our sample was able to demonstrate the efficacy of utilizing professional help to cope with the impact of COVID-19; this may provide evidence for other populations within the Muslim community that seeking mental healthcare is beneficial.

A masked woman bundled in winter clothes crosses an empty city street alone